I bought some more CRWD, ASND, PANW, UTHR and VGT.
These guys are doing really well.
But when in doubt, just buy Vanguard’s tech ETF called VGT. Each month put money into VGT, irrespective of its price. It’s called Dollar Cost Averaging. It works.
I put in a low $103.25 bid to buy Peloton (PTON). It’s becoming a service company, not a bicycle company. I think there’s a huge future in the “customized exercise classes taken n the home” market. Who wants to schlepp to a stinky, dirty, stuffy gym when you can exercise handsomely in your own stinky, dirty, stuffy basement?
Our stocks have exploded this week. I don’t know why. But I do know — You should always be fully invested. Cash is NOT king.
Tips
+ My Subaru Outback handles better when it has a full tank of gas. The extra weight helps hugely.
+ Airports and planes are full. My flights to and from the west were packed. I’m thinking double masks.
+ Do not plan on eating airline food. It’s truly gross — even in “first class.” A dead banana looks positively appealing compared to what they served me on Alaska’s “first class” from Portland to JFK.
+ Google finds instruction manuals for your latest gadget. Amazing how superb Google’s searching has become. They’re also doing good selling advertising, too.
+ Save your cell phone’s battery. Turn down the screen. Cut the number of apps running, especially Waze. Swipe up from the bottom halfway and then slide up the running apps.
+ Don’t give your email or phone number to anyone for any reason — like a discount. It’s not worth it. You’ll be bombarded with stuff you don’t need.
+ Collect the cell phone number of very technician who fixes something for you. Find out what he/she did. Tip them handsomely.
+ Plant based hamburgers taste awful — unless you smother them with something — anything.
+ Drink water. Eat less. Keep moving. Take naps.
What motivates a suicide bomber?
Three things:
+ They go to Heaven.
+ The family gets new stature in the community. Their son/daughter is a matryr, a hero.
+ In some places, your family will receive a handsome financial reward from the local government.
Frankly, I’m scared
I’m scared for my grandchildren. None are vaccinated. And there’s a whole bunch of idiot adults who won’t be vaccinated for whatever cockamamie reasons.
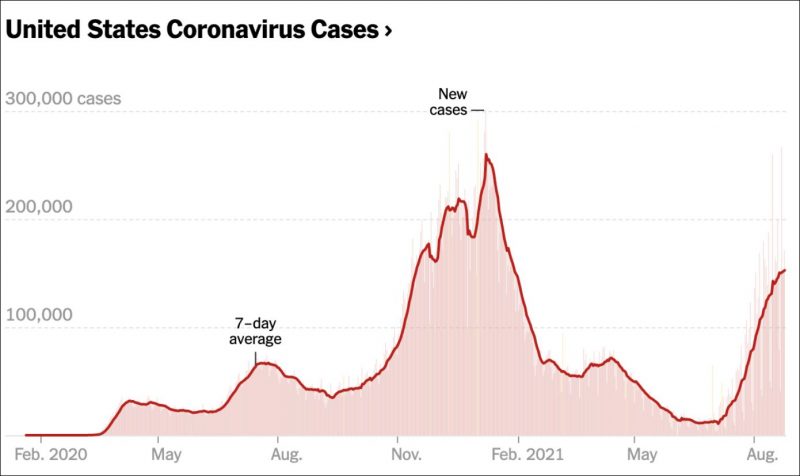
The Delta variant is making it worse. Once again, they’re using refrigerated trucks to store the dead bodies — unvaccinated idiots. And nobody can get a bed for elective surgery because all the beds are full with Covidees. This chart is so depressing:
Maybe you know of people who won’t be vaccinated because “the vaccines are unsafe.”
Here’s a beautiful New Yorker article by a Clayton Dalton, an emergency physician, who lives and works in New Mexico.
Why the COVID Vaccines Aren’t Dangerous
Many vaccine-hesitant people worry about adverse health effects. They shouldn’t.
As the Delta variant gains momentum around the country, I’m seeing more and more unvaccinated patients in my E.R. I often ask them why, after the devastation we’ve seen this year, they’ve chosen not to get vaccinated. Sometimes their answers are weird or conspiratorial. But most people say that they’re concerned about something real: adverse effects. They’ve heard about blood clots in women, or about myocarditis in young men, and the prospect of developing one of these frightening conditions has kept them away from the vaccination clinic. Recently, I spoke to two members of my extended family who hadn’t yet been vaccinated. They, too, cited adverse effects. They’re definitely not alone: a Census Bureau poll, conducted in late June and early July, found that a majority of unvaccinated respondents have avoided the vaccine because they are concerned about the risks.
I can understand their reticence; blood clots and inflamed hearts make me nervous, too. What they’re missing, however, is a proper context in which to understand the risks of the vaccines-as well as a sense of how risk fits into medicine more generally.
Nearly everything that doctors do carries risk. Surgeries can go awry. Diagnostic tests can yield false positives, exposing patients to more invasive tests or procedures. Medications and vaccines are no exception. Some 1.3 million emergency department visits are attributed to adverse drug effects each year, and studies have estimated that nearly seven per cent of hospitalized patients suffer some form of adverse drug reaction, with a fatality rate of 0.3 per cent. These numbers, extrapolated across the country’s population, suggest that more than two million adverse drug reactions probably occur in U.S. hospitals each year, potentially resulting in more than a hundred thousand deaths. If that’s true, then adverse drug effects are the fourth-leading cause of death in the United States-ahead of diabetes, pneumonia, and car accidents.
This all sounds quite risky. Does it mean that we should avoid prescription medicines entirely? Let’s look at the most common adverse-reaction offenders. Anti-seizure drugs, insulin, and blood-thinning medications-often used to prevent stroke-are at the top of the list; antibiotics account for more adverse effects than almost any other kind of drug, leading to approximately a hundred and fifty thousand E.R. visits annually; even acetaminophen turns out to be risky, causing fifty-six thousand E.R. visits, twenty-six hundred hospitalizations, nearly half of all liver failures, and over four hundred and fifty deaths each year. Nevertheless, I think that most of my vaccine-hesitant patients would agree that preventing strokes and seizures, treating diabetes, alleviating pain, and curing infections are extremely important, and that the benefits we derive from using these medications weigh favorably against their risks.
The lesson here is that treating illness is a complex undertaking, always freighted with a degree of uncertainty and risk. We know that medicines can heal as well as harm: the word “pharmacology” comes from the Greek pharmakon, which refers not just to healing medicines but also-in classic Greek-to deadly poisons. A few months ago, I took care of a woman who had been prescribed a common antibiotic for a skin infection. She came in a week later with kidney failure-a known but rare effect of the drug. I felt terrible about her outcome, but I still prescribe that medication. We can make educated guesses about who may be more at risk for a particular harm caused by a particular drug, and about how to measure that risk against the potential benefits. If I know that a patient already has kidney problems, I’ll choose a different antibiotic. Although we can never precisely predict who will be harmed, or how, the central effort is to figure as best we can the over-all balance of these various probabilities.
The practice of clinical medicine revolves around this aim. It is about bringing a fuzzy, multifaceted constellation of competing risks and benefits as sharply into focus as possible for an individual patient. When the doctor at the foot of your bed goes silent, she’s probably focussed on conjuring this calculus in her mind. The output-a kind of risk-benefit analysis based on the sum total of our education and experience-is what guides our decisions and recommendations. I explained this balancing act to another patient this month, when side effects for an antiviral medication brought her back to the E.R. The initial problem had been resolved, and now the adverse effects of the medicine outweighed the benefits. The balance had shifted, and I recommended that she stop taking it. “Oh,” she said, nodding. “Kind of like a teeter-totter.”
It is this weighing of risks and benefits, in all their many facets, that informs the chorus of health-care professionals imploring their families, neighbors, co-workers, and friends, along with everyone else, to please get vaccinated against covid-19. They urge vaccination because they see its ratio of risks to benefits as incredibly, unbelievably good. Better than over-the-counter pain relievers. Better than many antibiotics. Better than almost everything that we routinely order or prescribe in the E.R. Ninety-four per cent effective in preventing severe covid-19, hospitalization, and death? That was beyond my wildest dreams a year ago. Moreover, early data from the United Kingdom suggests that the vaccines remain highly effective in preventing these serious outcomes with the Delta variant. In the E.R., I often have to tell my patients that, unfortunately, we don’t have a silver bullet for what ails them. But, in the case of covid, we do. We have the silver bullet. Never mind the fact that this treatment in particular not only helps protect you as an individual but helps protect your loved ones, your community, the entire world. What other medical intervention even comes close?
And what about the risks? What goes on that side of the equation? In the spring, eighty-six potential cases of blood clots related to covid vaccination in Europe were reported, out of a total of twenty-five million vaccinations administered. In the United States, out of thirteen million doses administered, forty-two cases of blood clots have been associated with the Johnson & Johnson vaccine. That’s a rate of 0.0003 per cent. For the Moderna vaccine, the number of patients who suffered from blood clots so far is two. A study of the AstraZeneca vaccine, released late last month, found that, after the first dose, the rates of blood clots associated with vaccination were between two and eight per million recipients. covid, on the other hand, raised the risk of blood clots by eight hundred per cent.
The same pattern repeats itself for all of the vaccines’ adverse effects. A hundred and sixty-one cases of Guillain-Barré syndrome-a rare neurological condition that causes weakness-have been associated with the Johnson & Johnson vaccine, out of more than thirteen million doses administered. Nearly three hundred and fifty million doses of the Moderna and Pfizer vaccines have been given in the United States; so far, about seven hundred cases of myocarditis or pericarditis have been confirmed. Most of them were reported after the Moderna or Pfizer mRNA vaccine and the patients recovered within a few weeks. That’s about 0.0002 per cent of vaccine recipients. Can you even begin to imagine how small two or six or eight per million is? Or even seven hundred out of three hundred and fifty million? The population of the United States is about three hundred and twenty million. If seven hundred people, scattered all across the country, raised their hands, how long would it take for you to find them all?
For some people, it’s not so much the known risks that have them worried as the unknown. They ask, What if the mRNA vaccines alter our DNA, threatening our health far in the future? Will they affect our bodies in other, as yet undiscovered, ways? After all, some say, this is brand-new technology, and the F.D.A. has only fully approved the Pfizer vaccine.
As it turns out, though, mRNA technology isn’t especially new. Scientists have been developing it since the nineteen-nineties. And the principles behind it are startlingly simple and elegant. Most existing vaccines contain the actual virus that they are meant to protect against; some, like the polio vaccine, contain “killed” virus, which has been altered so that it cannot replicate in our cells, whereas others, like the measles vaccine, contain live “attenuated” virus, which can replicate but has been engineered to trigger an immune response rather than an infection. The mRNA vaccines are an improvement upon these shots, because they contain no virus at all. Instead, they consist of tiny packages that deliver a set of instructions to our cells. The instructions take the same form-messenger RNA-that all cells use to make each and every protein in our bodies. In the case of the covid vaccines, the instructions tell our cells how to make the spike protein, which is a single piece of the coronavirus that studs its outer capsule, like a flag. No other part of the virus is involved. Our cells recognize the spike protein as foreign, and display it to our immune system, which responds by preparing to fight off the actual virus. As soon as the mRNA blueprints are read, the cell destroys them. All of this happens outside of the cell nucleus, where our DNA is housed; it doesn’t interact with our DNA in any way. It’s a brilliant technique, and there’s no scientific basis for the idea that these vaccines might threaten our health in the future. Once they’ve done their job, they just disappear.
If it’s all so simple and safe, then why hasn’t the F.D.A. granted all of the vaccines full approval yet? It’s not because there isn’t enough safety data, or because of hidden concerns about additional health risks. “In the history of medicine, few if any biologics (vaccines, antibodies, molecules) have had their safety and efficacy scrutinized to this degree,” Eric J. Topol, the founder of Scripps Research Translational Institute, wrote recently, in the New York Times. The reason is that full approval for any medication requires a huge amount of paperwork, and a lot of field work, too. The F.D.A. already knows how rare the vaccines’ adverse effects are, but six months’ worth of data and documentation still has to be reviewed for each and every participant in the initial vaccine trials. “You have a lot more data to review than for an emergency use authorization,” Peter Marks, who oversees the approval process at the F.D.A., has said. “It’s going from tens of thousands of pages to hundreds of thousands of pages.” In addition, the F.D.A. has to conduct inspections of the production facilities where the vaccines are made, which are located in many different countries around the world. It’s an extremely laborious process, designed for slower-paced times-but it’s all in the name of safety. It’s an unfortunate irony that a process designed to instill confidence in approved treatments has, because of its incredible rigor, inspired doubts about the safety of the vaccines.
Many months into the vaccine rollout, in the midst of the Delta wave, it’s tempting to assume that positions have hardened, and that no one is capable of changing his or her mind. But it’s not too late, and it’s important to keep telling people not just that the vaccines are safe but why they are safe. Recently, I explained all of this to my reticent family members on the phone, and urged them to consider getting their shots. They said that they’d think about it. A few days later, they texted to say that they were leaning toward vaccination.
The above article came from here.
Son Michael jumping
He’s jumping into the Middle Fork of the Salmon River in Idaho while on the wonderful OARS trip we did recently. I did not jump. I shot this with my iPhone 12 Pro Max. Amazing scenery. Great river. Great guides.
Why I only have shares in Amazon — not FedEx or UPS
Don’t blame me for this silly video.
I played tennis this morning at 7:00 AM in Columbia County, NY. It was glorious.
Want to see how stupid the anti-vaxers are: Read a piece on CNBC.com today called “Clamoring for ivermectin, some turn to a pro-Trump telemedicine website.” Click here.
Don’t do stupid. And have a great weekend. — Harry Newton